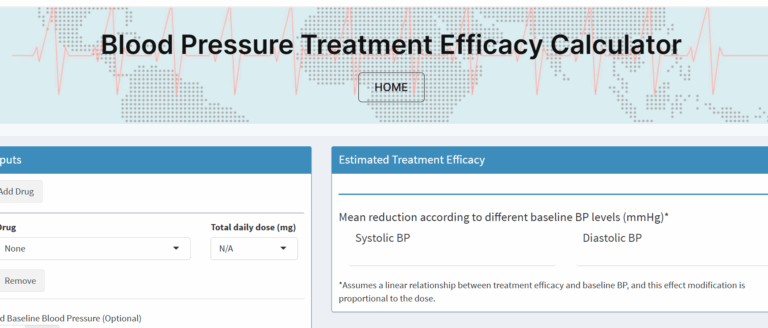
A new online blood pressure management tool helps doctors choose treatments that yield real blood pressure drops. It uses trial data to guide smarter care.
The 2025 AHA blood pressure guidelines bring important changes for patients. Risk scores, treatment thresholds, and lifestyle goals have all been updated. Learn what these changes mean for your daily care and long-term health.
Eating blood pressure friendly food is one of the five keys to an effective lowering of high blood pressure into the normal range. Learn from the practicing expert